
July 27, 2023
How our phage therapy system works at Phage Australia
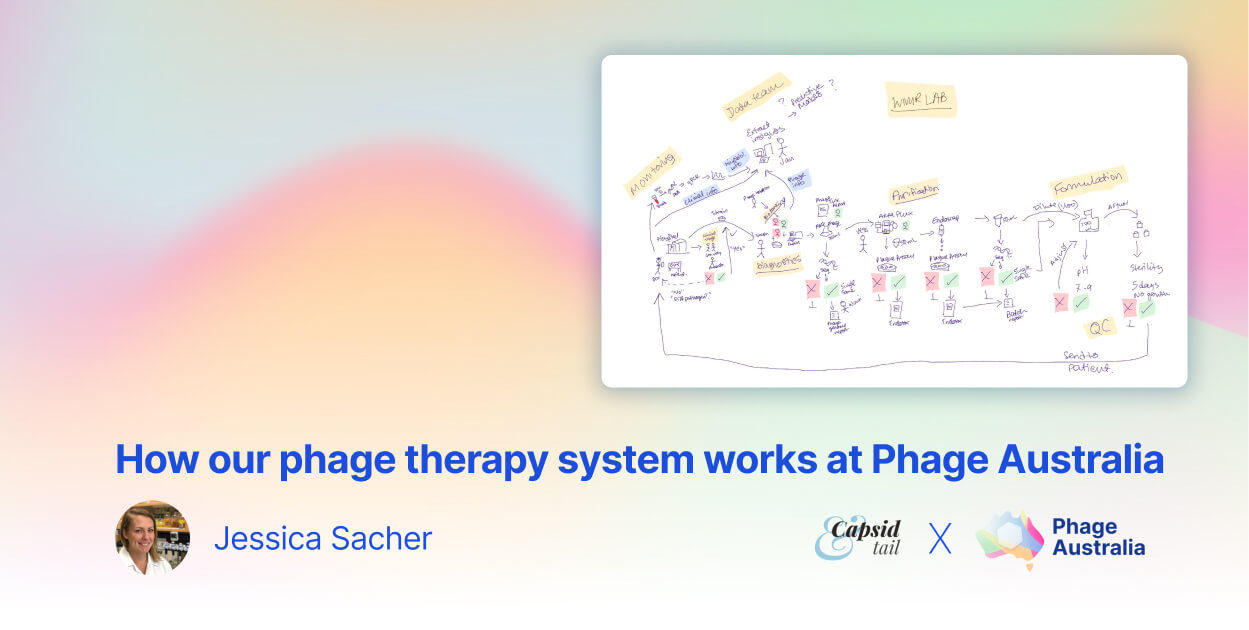
Blog PostAt Phage Australia, we’re scaling up personalized phage therapy. Here’s an overview of the process, to assist other centers in navigating the challenges of running a successful phage therapy (or other bio-based) service.